
Featured Site
Beyond the Horizon
This student-created digital exhibit showcases the lives of early women astronomy students at the Detroit Observatory. These pioneering women left a legacy that is as big as the cosmos itself.
Learn more

News
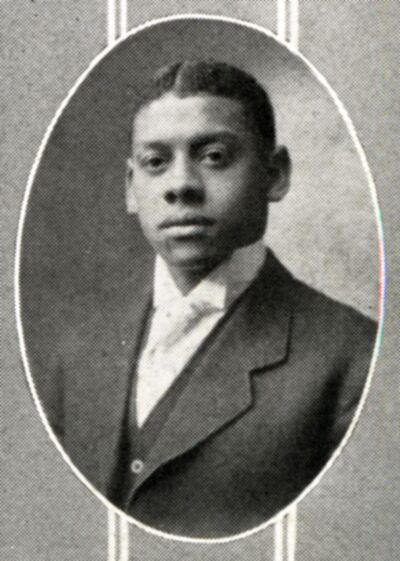
Strong as Steel
Cornelius L. Henderson was a pioneering steel engineer and architect who helped construct two of the major Great Lakes bridge crossings between the United States and Canada.
Complete Story
Stay Connected

Happy National Library Week! ⭐
Did you know that there are libraries on campus containing sheet music, or computer games, or ancient papyrus? 🤯
U-M has at least 20 different libraries, all of them with their own specialties and types of collections, including the Bentley! 📚📖💙
At the Bentley Historical Library we really love helping people dive into the history of U-M, and the state of Michigan, with things like:
📖 Scrapbooks from students long ago!
📸 Photographs of what your dorm looked like when it was first built!
🗺️ Old maps of the state of Michigan!
📽️ Videos of U-M weather experts sailing past icebergs!
🏈 Boxes full of football play-by-play game rundowns!
…And more!
Sometimes visitors see the word “library” on the Bentley’s sign, and assume our stacks are full of books.
We love books, and the Bentley contains plenty of them. But the truth is, we also have so much more to share!
We encourage you to come visit our Reading Room to find out more, and to check out U-M’s many libraries, to see everything they have to offer!
Click through to glimpse historic photos of just a few of the many wonderful libraries on U-M`s campus.
How many of them can you recognize?
#NationalLibraryWeek #Libraries #UMich #GoBlue #ReadingIsCool #SupportYourLocalLibrary
{kind=link}
Happy National Library Week! ⭐
Did you know that there are libraries on campus containing sheet music, or computer games, or ancient papyrus? 🤯
U-M has at least 20 different libraries, all of them with their own specialties and types of collections, including the Bentley! 📚📖💙
At the Bentley Historical Library we really love helping people dive into the history of U-M, and the state of Michigan, with things like:
📖 Scrapbooks from students long ago!
📸 Photographs of what your dorm looked like when it was first built!
🗺️ Old maps of the state of Michigan!
📽️ Videos of U-M weather experts sailing past icebergs!
🏈 Boxes full of football play-by-play game rundowns!
…And more!
Sometimes visitors see the word “library” on the Bentley’s sign, and assume our stacks are full of books.
We love books, and the Bentley contains plenty of them. But the truth is, we also have so much more to share!
We encourage you to come visit our Reading Room to find out more, and to check out U-M’s many libraries, to see everything they have to offer!
Click through to glimpse historic photos of just a few of the many wonderful libraries on U-M`s campus.
How many of them can you recognize?
#NationalLibraryWeek #Libraries #UMich #GoBlue #ReadingIsCool #SupportYourLocalLibrary
Happy National Pet Day! 🐶🐱💙
Click through to see pets from Michigan history, and the people who loved them.
Proof that the bond between a human and their pet is truly timeless! 🐾
📸: Dog and little girl in Chelsea, Michigan, from the Thomas Shaw papers
📸: Cat and boy, from the Emile Low scrapbook
📸: Girl with rabbits, from the Squier Family papers
#NationalPetDay #PetsOfInstagram #OldPhotos #Dog #Cat #Rabbits
{kind=link}
Happy National Pet Day! 🐶🐱💙
Click through to see pets from Michigan history, and the people who loved them.
Proof that the bond between a human and their pet is truly timeless! 🐾
📸: Dog and little girl in Chelsea, Michigan, from the Thomas Shaw papers
📸: Cat and boy, from the Emile Low scrapbook
📸: Girl with rabbits, from the Squier Family papers
#NationalPetDay #PetsOfInstagram #OldPhotos #Dog #Cat #Rabbits
On this day in 1899, “The Victors” was played for the very first time! 🥳
“Hail to the victors valiant, hail to the conquering heroes…” 🎵
You’ve probably heard U-M’s iconic song, “The Victors,” played at football games before. 🏈
But did you know that it was inspired by one?
In 1898, U-M student Louis Elbel watched the Wolverines defeat the Chicago Maroons 12 to 11, ending a victorious football season!
Elbel was so inspired by the game that, on the train ride back to Ann Arbor, he worked on writing a song that would soon be known as “The Victors.” 🚂
On April 5, 1899, according to the Michigan Daily, a student orchestra led by Elbel played “The Victors” for the very first time in public, as part of a student play titled, “A Night Off.”
The audience loved it so much, they asked for an encore.
Little did they know that this song was history in the making, soon to be beloved by fans around the world!
If you’re curious to learn more about that first performance of “The Victors,” check out the Michigan Daily Digital Archives.
Be sure to also check out @umichband to watch a video of the band playing “The Victors” in the modern day! 🎺
#OTD #UMich #GoBlue #Wolverines #TheVictors #LouisElbel #MarchingBand #FootballHistory
{kind=link}
On this day in 1899, “The Victors” was played for the very first time! 🥳
“Hail to the victors valiant, hail to the conquering heroes…” 🎵
You’ve probably heard U-M’s iconic song, “The Victors,” played at football games before. 🏈
But did you know that it was inspired by one?
In 1898, U-M student Louis Elbel watched the Wolverines defeat the Chicago Maroons 12 to 11, ending a victorious football season!
Elbel was so inspired by the game that, on the train ride back to Ann Arbor, he worked on writing a song that would soon be known as “The Victors.” 🚂
On April 5, 1899, according to the Michigan Daily, a student orchestra led by Elbel played “The Victors” for the very first time in public, as part of a student play titled, “A Night Off.”
The audience loved it so much, they asked for an encore.
Little did they know that this song was history in the making, soon to be beloved by fans around the world!
If you’re curious to learn more about that first performance of “The Victors,” check out the Michigan Daily Digital Archives.
Be sure to also check out @umichband to watch a video of the band playing “The Victors” in the modern day! 🎺
#OTD #UMich #GoBlue #Wolverines #TheVictors #LouisElbel #MarchingBand #FootballHistory
Throwback to Ann Arbor over 100 years ago! 🕜
Click through to see photos from Ann Arbor as it looked in the year 1914, including:
🚘 A sunny day on State Street
🌳 A beautiful view across Ann Arbor from “The Boulevard”
🌊 U-M students competing in tug-of-war across the Huron River
🔧 The construction of bleachers at Ferry Field, where many early football games were played
🏠 One of the oldest buildings still on campus: the U-M Presidents’ House
The same year that these photographs were taken, Babe Ruth debuted in major league baseball, construction had just started on the Lincoln Memorial, and World War I began.
When people think back to 2024 in the future, what do you think they’ll remember?
📸: Images sourced from the Photograph Vertical Files, Athletic Department Records, and Sam Sturgis Photographs
#TBT #AnnArbor #UMich #HuronRiver #FerryField #MichiganHistory
{kind=link}
Throwback to Ann Arbor over 100 years ago! 🕜
Click through to see photos from Ann Arbor as it looked in the year 1914, including:
🚘 A sunny day on State Street
🌳 A beautiful view across Ann Arbor from “The Boulevard”
🌊 U-M students competing in tug-of-war across the Huron River
🔧 The construction of bleachers at Ferry Field, where many early football games were played
🏠 One of the oldest buildings still on campus: the U-M Presidents’ House
The same year that these photographs were taken, Babe Ruth debuted in major league baseball, construction had just started on the Lincoln Memorial, and World War I began.
When people think back to 2024 in the future, what do you think they’ll remember?
📸: Images sourced from the Photograph Vertical Files, Athletic Department Records, and Sam Sturgis Photographs
#TBT #AnnArbor #UMich #HuronRiver #FerryField #MichiganHistory